Endodontics
This page contains the documents that relate to the Dental Specialty Fellowship Examinations for this topic.
- Examination Syllabus
- Assessment strategy
- Link to the GDC Curriculum
- Link to the training syllabus defined by the Specialty Advisory Committee (SAC)
- Illustration of how the change to the curriculum impacts the examination certifications
- Part 1 SBA Sample Questions
Examination Syllabus
Assessment Strategy
GDC Curriculum and Training Syllabus


Training syllabus – As defined by the Specialty Advisory Committee (SAC)
Illustrative Examination Route
The image below is to illustrate the changes to certification as a result of the introduction of the new curriculum. The illustration assumes full time training. Trainees on the NTN pathway should refer to their TPD’s or Post Graduate Dental Dean for information about progression.
Sample Questions
Below are five sample Single Best Answer (SBA) questions selected from across the syllabus. These questions are designed to be indicative of the level, style, and cognitive demand of the examination and reflect the use of higher‑order clinical reasoning. They are provided solely as a guide and should not be interpreted as representative of the full breadth or specific content of the assessment.
You will be required to select the most appropriate answer from a choice of five answers. There may be images and/or test results included in the data provided for the question.
The examination comprises two papers of 90 SBA questions, each of two hours’ duration. There is no negative marking, and candidates are therefore encouraged to attempt every question. During each paper, candidates will be able to navigate freely between questions and amend their answers at any point prior to submission. Further information on the in-centre assessment experience will be made available on the website and in direct communications to registered candidates.
Question 1
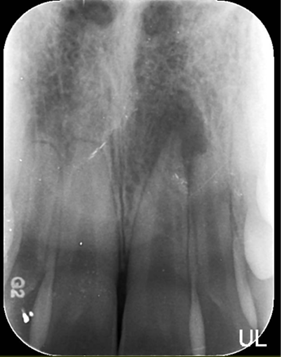
A 14-year-old patient attends their first appointment of regenerative endodontic treatment for a traumatised upper central incisor with asymptomatic apical periodontitis. A pre-operative radiograph is shown. Local anaesthesia is achieved with 3% mepivacaine hydrochloride (without adrenaline) and irrigation is performed with 3% sodium hypochlorite. During treatment, there is profuse bleeding into the canal, and the patient reports severe pain despite local anaesthesia.

What is the most likely cause of this event?
- Apical overpreparation
- Perforation
- Root fracture
- Sodium hypochlorite incident
- Poor anaesthesia
The correct answer is D.
Justification: The most likely cause is a sodium hypochlorite incident. The key clues are the open apex, irrigation with 3% sodium hypochlorite, sudden severe pain despite local anaesthesia, and profuse bleeding into the canal. Together, these are characteristic of inadvertent sodium hypochlorite extrusion beyond the apex with acute tissue injury. As this is the first visit for RET, apical over-preparation to induce bleeding should not have been performed. Perforation and root fracture may increase the possibility of sodium hypochlorite incident, but in isolation would not result in the symptoms described within the stem.
Question 2
A 14-year-old patient with ADHD has a discoloured UL1 with asymptomatic apical periodontitis. They are being managed using intravenous sedation. After access and thorough chemomechanical preparation with 3% sodium hypochlorite using passive ultrasonic irrigation, the canal is dry without exudate and working length is confirmed with a radiograph at 22 mm. An ISO 80 K file is the first file to bind at the working length. A pre-operative periapical radiograph is provided.
What is the most appropriate next step in management?
- Induce apical bleeding to commence regenerative endodontic treatment
- Place 4 mm of calcium silicate cement to create an apical barrier
- Place an intracanal medicament and review healing
- Obturate with thermoplasticised gutta-percha to full working length
- Seal the root canal system and place 16% carbamide peroxide into the pulp chamber
The correct answer is B.
Justification: This stem and radiograph demonstrate an immature but relatively advanced (Cvek stage IV) incisor. Access, irrigation, and working length confirmation have already been completed and the canals have been confirmed as dry and free from exudate. The next step is to establish an apical barrier using a calcium silicate cement. RET is a plausible distractor because it is an accepted option for some immature necrotic teeth, but it is generally favoured in more immature teeth, especially when further root maturation is a realistic objective. Review literature states that RET is mainly recommended for Cvek stages I–III, whereas teeth with near or more advanced root formation are more suited to conventional treatment or hydraulic calcium silicate barrier techniques. Whilst conventional obturation would also be feasible and plausible, it is not considered best practice in large apices. Intracanal dressing may be appropriate in specific cases where infection remains or canals cannot be dried but should be avoided where possible in a young patient being managed under intravenous sedation where calcium silicate cement is being used. Carbamide peroxide should be reserved for post-obturation and would likely follow the correct answer.
Question 3
A previously root-filled UR2 has a persistent sinus tract. A GP-tracing radiograph is taken and shown. Root canal retreatment is performed, but the apical gutta percha cannot be retrieved and the sinus tract fails to resolve. The adjacent UR3 is vital. Apical surgery is performed and histopathology of the curetted tissues shows branching filamentous gram-positive organisms with radiating eosinophilic club-shaped peripheral structures.

What is the most appropriate interpretation of the histopathology in this case?
- Foreign-body reaction to extruded root filling material
- Periapical actinomycosis, causing persistent extraradicular infection
- Radicular cyst with cholesterol clefts
- Chronic apical abscess caused by persistent intraradicular infection
- Lateral periodontal cyst from the UR3
The correct answer is B.
Justification: Periapical actinomycosis, causing persistent extraradicular infection Branching filamentous gram-positive organisms are classic histopathological features of actinomyces. Radiating eosinophilic club-shaped peripheral structures describes the Splendore–Hoeppli phenomenon, producing the classic appearance of sulfur granules. In a previously treated tooth with persistent apical disease and a sinus tract, this most strongly supports periapical actinomycosis, an extraradicular infection associated with persistent apical periodontitis. Histopathological studies of periapical lesions identify these staining features as indicative of actinomyces, and endodontic literature describes periapical actinomycosis as a cause of persistent disease despite prior root canal treatment.
Question 4
A 54-year-old patient has mild pain from their UL1. The tooth is tender to percussion, is Grade 1 mobile and has an isolated 6 mm mesiopalatal probing defect. There is light intercuspal position contact on the UL1 with protrusive guidance on the UR1. The periapical radiograph recorded is shown.

What is the most appropriate definitive management for the UL1?
- Extraction
- Endodontic microsurgery
- Root canal retreatment
- Intentional re-implantation
- Occlusal adjustment
The correct answer is A.
Justification: The combination of a previously traumatised, root-treated anterior tooth with an isolated deep periodontal probing defect is highly indicative of a vertical root fracture. The tooth is mobile and tender to percussion with radiographic evidence of a wide tapered post, periodontal bone loss and an over-extended root canal filling. Endodontic microsurgery would leave minimal remaining periodontal support and worsening mobility. In this context, prognosis is poor and extraction is the most appropriate definitive management.
Question 5
A 42-year-old patient is referred after their GDP could not negotiate the LR5 canal beyond the mid-root. The periapical radiograph taken is shown.
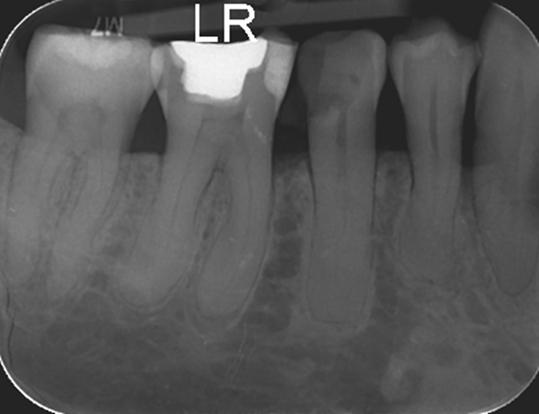
What is the most likely explanation for the radiographic appearance of the root canal system in the apical half of the root?
- Bifurcation of the root canal system
- Hyper-cementosis, causing apical canal obliteration
- Ledge formation in the mid-root
- Taurodontism
- Tertiary dentine deposition, causing progressive calcific narrowing
The correct answer is A.
Justification: This is the classic fast break pattern: the canal is visible in the coronal third and then shows a sudden narrowing or disappearance in the mid-root/apical half. In mandibular premolars, that radiographic sign suggests the canal is dividing into two branches or that additional canal anatomy is present. The referral history supports this: failure to negotiate beyond the mid-root is a common consequence of unrecognised bifurcation rather than simple calcification or access error. Literature on variable root canal anatomy states that a sudden change in radiographic density, narrowing, or disappearance of the pulp space usually indicates an additional canal or canal bifurcation.